Collider bias is an under-appreciated source of distortion in research, and there seems to be quite a lot of it in the deluge of COVID-19 literature. Oxford CEBM’s Catalogue of Bias has an excellent article on collider bias here:
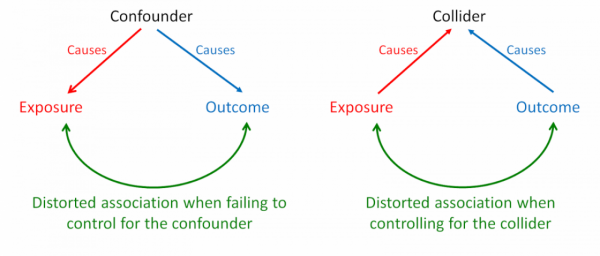
“When an exposure and an outcome independently cause a third variable, that variable is termed a ‘collider’. Inappropriately controlling for a collider variable, by study design or statistical analysis, results in collider bias. Controlling for a collider can induce a distorted association between the exposure and outcome, when in fact none exists. This bias predominantly occurs in observational studies. Because collider bias can be induced by sampling, selection bias can sometimes be considered to be a form of collider bias.”
Fortunately, a recent preprint highlights collider bias in COVID-19 research; “Collider bias undermines our understanding of COVID-19 disease risk and severity.” One of the authors, Tim Morris, has a great, informative twitter thread on their findings below (click the tweet to see the full thread):
A few of us at the @mrc_ieu have a preprint discussing collider bias with a focus on coronavirus research. We're of the opinion that collider bias is a big banana skin that a lot of studies may be stepping on. A brief thread (1/20)…https://t.co/ZUDMvxozAA #COVID19 #epitwitter
— Tim Morris (@bristimtom) May 10, 2020
[1] Griffith, G., Morris, T. T., Tudball, M., Herbert, A., Mancano, G., Pike, L., Sharp, G. C., Palmer, T. M., Davey Smith, G., Tilling, K., Zuccolo, L., Davies, N. M., & Hemani, G. (2020). Collider bias undermines our understanding of COVID-19 disease risk and severity. Cold Spring Harbor Laboratory. doi: 10.1101/2020.05.04.20090506